
Adaptation. This has been defined as a change or the process of change by which an organism or species becomes better suited to its environment.
This is what living organisms do – they adapt. And perhaps there is no better example of this than the response to exercise. When we exercise, we can become bigger, faster, and stronger. Similarly, however, we can become fatter, slower, and weaker if we don’t move and indulge in caloric excess.
If you really think about it, this is pretty amazing. Our bodies are remarkably dynamic and our minds are much the same.
And while it’s easy for us to consider the adaptive response of a bigger bicep or a wider waistline, there are endless examples. I wrote about tendon responses to loading in the previous article series on tendon injuries (October – December 2017).
But let’s consider bones. If you want to read about some crazy cases of bony adaptation, dig up a copy of the 1822 book, A Treatise on Dislocations and Fractures of The Joints. In it, Sir Astley Cooper, an English surgeon and anatomist, reports cases of anatomic adaptations to chronically dislocated or fractured bones. Imagine; it’s pre-1822 so not much can be done about some pretty horrific injuries.

In one case, Sir Astley Cooper describes anatomic changes that occur from chronic dislocation of the hip joint:
“The pressure of the head of the bone produces absorption…a smooth hollow surface is formed, and the ball becomes altered in its shape to adapt it to this new surface…a deep cup is formed to receive the head of the bone; and perhaps no instances can be adduced which more strongly mark the powers of nature in changing the form of parts to accommodate them to new circumstances, than these effects of dislocation.
The new cup which is thus formed, sometimes so completely surrounds the neck of the bone, as to prevent its being separated without fracture and the socket is smoothed upon its internal surface, so as to leave no projecting parts which can interrupt the motion of the bone in its new situation.”
There are similar reports of shoulder dislocation. When the humeral head rests against a flat portion of the scapula rather than its native glenoid, a new socket is eventually formed. In fact, such a case has been described in which the new joint orientation served as a functioning shoulder joint for over 50 years! Have you ever seen a tree grow around a fence? It’s a similar phenomenon.
The remodeling of bone in response to loading is achieved through mechanotransduction – a process through which mechanical signals/forces are converted into biochemical signals in cellular signaling.

This remodeling was famously described by Julius Wolff, a German surgeon and anatomist, who in the 19thcentury stated that the repetitive loading of bone will cause adaptive responses enabling the bone to better cope with these loads. This became known as Wolff’s law. The stronger bones in the racquet-holding arm of tennis players and the generally increased bone density in weightlifters further exemplify it.

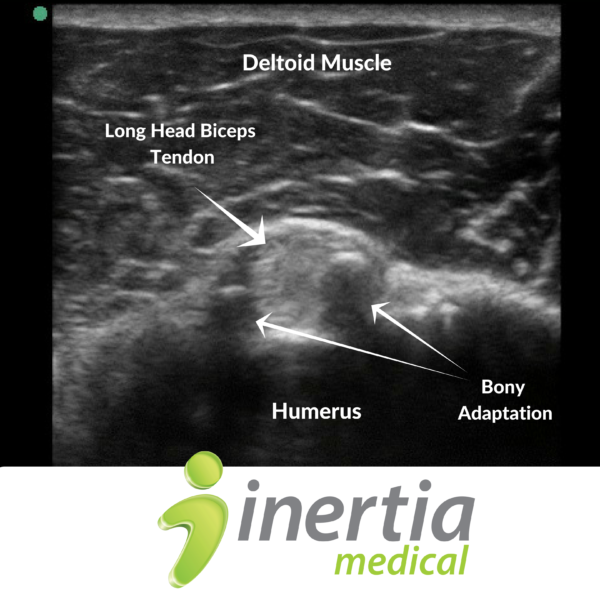
Speaking of weightlifters, I was reminded of bone remodeling while performing a shoulder ultrasound examination on IFBB professional bodybuilder, Blair Mone. In each of our shoulder joints, the long head of the biceps tendon sits in a fairly shallow groove on the anterior aspect of the arm bone. This is called the bicipital groove. Given the large size of Blair’s bicep tendon and the immense amount of tension carried through the tendon during his training sessions, the borders of the groove (the greater and lesser tubercles) have grown in such a way as to resemble pillars of bone in order to keep the tendon seated within the groove. It’s pretty wild, I must say.

And though fortification and formation of bone is an appropriate response to repetitive stress and patterns of loading, there are examples of when this is perhaps less favorable, as in cases of osteoarthrosis. While the development of osteoarthrosis is multifactorial and involves changes in many elements of joint tissue, bone remodeling seems to be a highly implicated part of the disease process. An injury, peculiar joint alignment, and generally altered mechanics can lead to abnormal load distribution across a joint and therefore result in overburdening of particular regions of bone. This causes several properties of the bone to change. These include expanding subchondral bone cross-sectional area, changes in bone mass, and remodeling of the trabeculae network. These changes likely lead to maladaptive responses in other articular structures, most notably cartilage. For instance, animal studies have demonstrated that surgical damage to subchondral bone leads to degradation in the overlying articular cartilage. This may occur in part via impaired flow of nutrients to the avascular hyaline cartilage via the altered cartilage-bone interface. It is also possible that, as bone area expands, cartilage begins to thin, leading to fissuring and further mechanical alteration. What’s the bottom line here? We need to be more mindful of mechanics and our patterns of movement. The adaptations described above are the result of repetitive stimulus – the application of load in a particular way over time. Is your form sloppy in the gym? It’ll catch up to you. Do you tend to carry things with the same arm or always bend to the same side in order to pick things up off the floor? Consider doing the opposite. Do you sit on a wallet in your back pocket? Don’t. When we are more mindful of our mechanics, we begin to move in a way that promotes tissue health and optimal function.


{kind=link}